I
I admit, when I heard about Robin Williams, I was shocked. Based on the reactions on social media, I was not alone.
Suicide (also called intentional self-harm) the number 10 leading cause of death in the US according to the Center for Disease Control.1 Much of the material for suicide and suicide prevention focuses on adolescents and young people, and for good reason. It is the second and third leading cause of death among young people, aged 15 to 34 years, surpassed only by accidental injury. And for every suicide completion, there are many more adolescents that attempt suicide. The prevalence of suicidal thoughts, suicide planning, and suicide attempts is significantly higher among young adults aged 18-29 years. By the time a person reaches 55 to 64 years, suicide has dropped to the eighth leading cause of death.
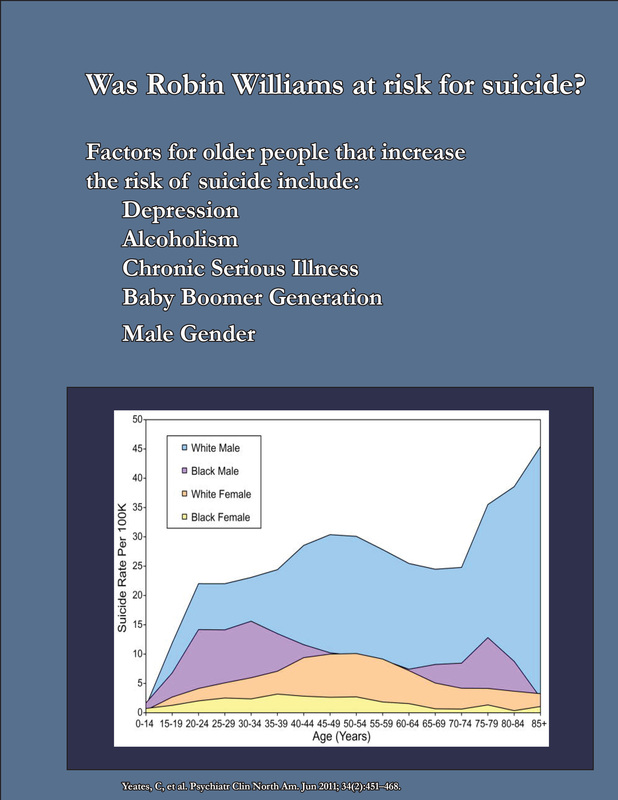
Perhaps that is why we were all so shocked. But should we have been? Buried deep within the data of suicide statistics is a terrible secret. While the above focuses on young people, the truth is this: Suicide rates at 36 per one hundred thousand, are the highest among men aged 75 years or older,2 even greater than young men (see chart below)2. Put another way, if you know about three thousand people over the age of 74, either in person, or online, or as a celebrity, you have a very good chance of knowing someone who will commit suicide as an older adult.
Robin Williams was a bit younger than this group of adults at 63 years of age, but the generation of “baby boomers” has had a proportionally higher suicide rate compared to the generations before and after.2 It was known that Mr. Williams was suffering from Major Depressive Disorder, an illness commonly found among post-mortem examinations in suicide completers.2 Other neurological disorders or mental illnesses associated with suicide completion include bipolar, psychotic disorders, ADHD, and schizophrenia, as well as anxiety.2
Reports also have been made that Mr. Williams was in the early stages of Parkinson’s disease, a chronic, progressive debilitating disease. Dr. Juurlink et al, reported in the Archives of Internal Medicine, that risk of suicide in patients 65 and older with illness is particularly high for those who have recently visited a doctor and/or had multiple illnesses.3 In addition, severe pain in particular, is a much greater risk factor for men than women, according to the Juurlink study (Odds ration of 9.9 vs. 3.3).3 Mr. Williams had open-heart surgery several years ago, and heart disease is heavily linked to depression in and of itself.4
The disparity between genders begs the question of what role masculinity and traditional gender roles play in suicide risk in older men. Some studies have shown that indeed, the traditional gender roles that position men as “the strong and silent type” increase the risk of suicide in elderly men (it is interestingly, somewhat different for younger men).5,6 This may be aggravated with the tendency for males to abuse alcohol as a way of coping with stress, as many suicide completers are found with alcohol in their system (other drugs noted at high prevalence include acetaminophen, opioids and antidepressants).7 Also present is the tendency to not discuss depression, so that even those closest to the man at risk may not be aware.8 Though it’s hard to imagine a man who had one of his most successful movies dressing up as a woman, to be struggling with masculinity issues, it is well-known that Mr. Williams had trouble with alcohol use.
Indeed all these factors put Robin Williams at risk of becoming another suicide statistics. Of what happened in those final, fateful moments, we may never know.
“Failures plagued me. Things I had omitted or ignored, neglected. What I should have given and hadn’t. I felt the biting pang of every unfulfillment.”
― Richard Matheson, What Dreams May Come
1. http://www.cdc.gov/violenceprevention/pdf/Suicide-DataSheet-a.pdf
2. Yeates, C, et al. Psychiatr Clin North Am. Jun 2011; 34(2):451–468.
3. Juurlink DN, et al. Arch Intern Med. 2004 Jun 14;164(11):1179-84.
4. Su, S, et al. Psychosom Med. 2009 Feb;71(2):152-8.
5. Hunt, K, et al. Soc Psychiatry Psychiatr Epidemiol. 2006 Aug;41(8):641-7. Epub 2006 May 26.
6. Möller-Leimkühler AM. Eur Arch Psychiatry Clin Neurosci. 2003 Feb;253(1):1-8.
7. Jones, AW. J Forensic Leg Med. 2013 Oct;20(7):842-7.
8. Brownhill S, et al. Aust N Z J Psychiatry. 2005 Oct;39(10):921-31.
I admit, when I heard about Robin Williams, I was shocked. Based on the reactions on social media, I was not alone.
Suicide (also called intentional self-harm) the number 10 leading cause of death in the US according to the Center for Disease Control.1 Much of the material for suicide and suicide prevention focuses on adolescents and young people, and for good reason. It is the second and third leading cause of death among young people, aged 15 to 34 years, surpassed only by accidental injury. And for every suicide completion, there are many more adolescents that attempt suicide. The prevalence of suicidal thoughts, suicide planning, and suicide attempts is significantly higher among young adults aged 18-29 years. By the time a person reaches 55 to 64 years, suicide has dropped to the eighth leading cause of death.
Perhaps that is why we were all so shocked. But should we have been? Buried deep within the data of suicide statistics is a terrible secret. While the above focuses on young people, the truth is this: Suicide rates at 36 per one hundred thousand, are the highest among men aged 75 years or older,2 even greater than young men (see chart below)2. Put another way, if you know about three thousand people over the age of 74, either in person, or online, or as a celebrity, you have a very good chance of knowing someone who will commit suicide as an older adult.
Robin Williams was a bit younger than this group of adults at 63 years of age, but the generation of “baby boomers” has had a proportionally higher suicide rate compared to the generations before and after.2 It was known that Mr. Williams was suffering from Major Depressive Disorder, an illness commonly found among post-mortem examinations in suicide completers.2 Other neurological disorders or mental illnesses associated with suicide completion include bipolar, psychotic disorders, ADHD, and schizophrenia, as well as anxiety.2
Reports also have been made that Mr. Williams was in the early stages of Parkinson’s disease, a chronic, progressive debilitating disease. Dr. Juurlink et al, reported in the Archives of Internal Medicine, that risk of suicide in patients 65 and older with illness is particularly high for those who have recently visited a doctor and/or had multiple illnesses.3 In addition, severe pain in particular, is a much greater risk factor for men than women, according to the Juurlink study (Odds ration of 9.9 vs. 3.3).3 Mr. Williams had open-heart surgery several years ago, and heart disease is heavily linked to depression in and of itself.4
The disparity between genders begs the question of what role masculinity and traditional gender roles play in suicide risk in older men. Some studies have shown that indeed, the traditional gender roles that position men as “the strong and silent type” increase the risk of suicide in elderly men (it is interestingly, somewhat different for younger men).5,6 This may be aggravated with the tendency for males to abuse alcohol as a way of coping with stress, as many suicide completers are found with alcohol in their system (other drugs noted at high prevalence include acetaminophen, opioids and antidepressants).7 Also present is the tendency to not discuss depression, so that even those closest to the man at risk may not be aware.8 Though it’s hard to imagine a man who had one of his most successful movies dressing up as a woman, to be struggling with masculinity issues, it is well-known that Mr. Williams had trouble with alcohol use.
Indeed all these factors put Robin Williams at risk of becoming another suicide statistics. Of what happened in those final, fateful moments, we may never know.
“Failures plagued me. Things I had omitted or ignored, neglected. What I should have given and hadn’t. I felt the biting pang of every unfulfillment.”
― Richard Matheson, What Dreams May Come
1. http://www.cdc.gov/violenceprevention/pdf/Suicide-DataSheet-a.pdf
2. Yeates, C, et al. Psychiatr Clin North Am. Jun 2011; 34(2):451–468.
3. Juurlink DN, et al. Arch Intern Med. 2004 Jun 14;164(11):1179-84.
4. Su, S, et al. Psychosom Med. 2009 Feb;71(2):152-8.
5. Hunt, K, et al. Soc Psychiatry Psychiatr Epidemiol. 2006 Aug;41(8):641-7. Epub 2006 May 26.
6. Möller-Leimkühler AM. Eur Arch Psychiatry Clin Neurosci. 2003 Feb;253(1):1-8.
7. Jones, AW. J Forensic Leg Med. 2013 Oct;20(7):842-7.
8. Brownhill S, et al. Aust N Z J Psychiatry. 2005 Oct;39(10):921-31.
 RSS Feed
RSS Feed
